

")
by The Honourable Brian Peckford
July 23, 20222
I Am In Shock

Jul 22, 2022
The United States Food and Drug Administration (US-FDA) had requested 75 years to release the documents that they reviewed from Pfizer prior to issuing emergency use authorization for the Pfizer-BioNTech BNT162b mRNA ‘vaccine’ (Comirnaty) against SARS-CoV-2, which can cause COVID-19. However, a judge over-ruled this and issued a court order that the documents be released in large monthly installments. Today, an absolutely shocking set of data were brought to my attention. They are not new. They are from a document that was in the data dump released back in May of this year. However, I want to help my fellow scientists in making sure that this science gets widely distributed throughout the world. This is for the sake of ‘fully informed consent’, something that regulatory agencies, public health officials and too many physicians seem to have abandoned over the past couple of years.
For a long time I have been arguing that our children need to be left out of the massive conflicts over the science underpinning COVID-19. In my opinion, adults can conduct their own risk-benefit analyses regarding whether they want to receive one of the current COVID-19 inoculations. However, far too many adults are making these decisions based on pseudo-science, data from flawed studies, misinformation, and outright disinformation being propagated by physicians and public health officials, many of whom are unqualified to opine on anything in the field of vaccinology. I have never felt comfortable about these injections being used in ‘children, adolescents and young-adults of child-bearing age’. This was the precise terminology I used in a parent’s guide to COVID-19 vaccines that I wrote more than one year ago.
COVID Chronicles is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
The highest quality data for assessing a novel medical product are derived from clinical studies. This is because these types of experiments in people are typically well-controlled and include what is known as ‘active monitoring’; there is follow-up to assess safety and efficacy. This is why the clinical testing phases should never be compromised. With this in mind, let’s explore a stunning set of data that Pfizer provided to the US-FDA. Here is the relevant document…
The data in this document were accumulated up until February 28, 2021. Notably, on page 9, safety concerns based on the US Pharmacovigilance Plan included “missing information” on “Use in Pregnancy and lactation”. The data that had accumulated up to the end of February, 2021 were from too small of a sample size (i.e., # of pregnant or lactating women) to justify its use in these populations. However, here are the data that were available at that time regarding outcomes in pregnant women that had received Pfizer’s COVID-19 inoculation; this is quoted from the top of table 6 (I have italicized and/or bolded the most important points)…
Pregnancy cases: 274 cases including:
• 270 mother cases and 4 foetus/baby cases representing 270 unique pregnancies(the 4 foetus/baby cases were linked to 3 mother cases; 1 mother case involved twins).
• Pregnancy outcomes for the 270 pregnancies were reported as spontaneous abortion (23), outcome pending (5), premature birth with neonatal death, spontaneous abortion with intrauterine death (2 each), spontaneous abortion with neonatal death, and normal outcome (1 each). No outcome was provided for 238 pregnancies (note that 2 different outcomes were reported for each twin, and both were counted).
Apparently, outcomes will never be known for 88% (238/270) of the pregnancies. Why was the follow-up rate on these cases so abysmal?
NutriTruth has a great graph on their website that summarizes the results from cases for which follow-up data were available…
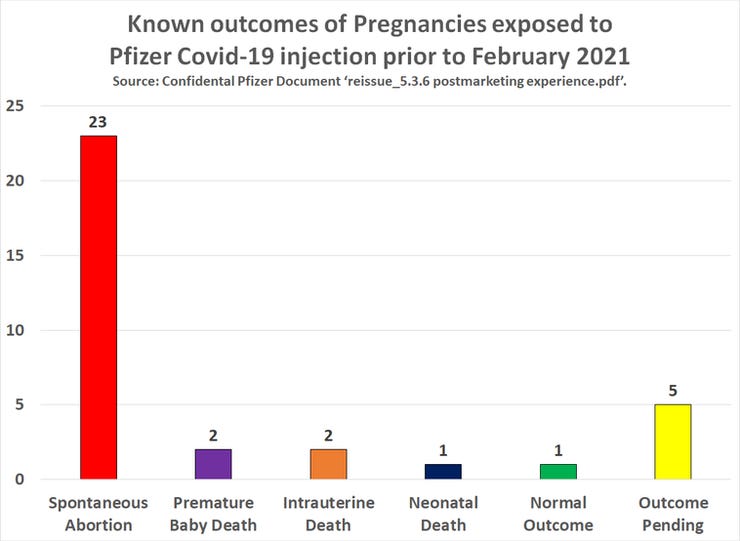
It appears that data would be available for five of the pregnancies, but these outcomes were still unknown at the time that Pfizer’s document was written. As such, there are solid data available from 29 pregnancies. One out of 29 of these pregnancies resulted in a ‘normal’ outcome. This means that 28 out of the 29 babies died! That is a 97% death rate. I don’t care which trustworthy data set you look at to determine a ‘background’ death rate, none of them come close to 97%. Spontaneous abortions are more common than many people appreciate, but, again, they are nowhere near the rate in this study. Even in the case of the ‘normal outcome’, this means there was an apparently healthy baby. However, one cannot be certain that the outcome was ‘normal’, until the baby has had all of their physiological systems fully mature, which means early adulthood.
I have looked at Pfizer’s pre-clinical reproductive toxicity data and they are fatally flawed. Issues included ‘vaccinating’ the females only; apparently it was forgotten that ‘it takes two to tango’. Also, the rodent models that were used express the low-affinity version of the receptor for the spike protein encoded by the ‘vaccines’. People express the high-affinity receptor. This means the rodent models aren’t capable of revealing toxicities that might be associated with the spike protein. In short, the pre-clinical studies could provide no assurance whatsoever that Pfizer’s vaccine would be safe in the context of pregnancy. Now there is proof that data were in the hands of regulatory agencies that suggested the potential for a 97% fatality rate for babies from ‘vaccinated’ women.
I have collaborated with scientists and physicians about the post-rollout ‘real-world’ studies on pregnancy and the COVID-19 shots. They are highly flawed. I co-authored a paper about this, but have yet to find an editor that will even allow it to undergo peer review (I have had no problems with this for any of my cancer- or basic virology-focused papers). Regardless, many other reputable scientists and physicians have been addressing this. Further, these ‘real-world’ studies should never have been authorized based on the data presented here.
Many countries have pushed Pfizer’s COVID-19 ‘vaccine’ on pregnant women, often via mandates. This was been done with the full blessing of their societies for obstetrics and gynecology. Are obstetricians and gynecologists going to continue to make these recommendations with these data in-hand? At the end of the day, couples experiencing pregnancies or who wish to do so must make it their own responsibility to educate themselves to facilitate fully informed consent. Too many obstetricians and gynecologists are either too superficially trained in the immunological sub-discipline of vaccinology or are too afraid of contradicting a narrative for which dissent is punished. Some physicians are starting to speak up about this. Unfortunately, their singular personal observations are simply deemed anecdotal. However, as a scientist, I have been trained to observe the cumulative nature of these reports; to not dismiss them out-of-hand, and to use them to formulate legitimate scientific questions.
If you or your baby have experienced any issues post-inoculation, please report these to your physician. They are obligated to submit an adverse event report, without opining on whether or not they think it might or might not be related. The accumulation of these reports is the only way scientists can help identify safety signals during a public rollout of a novel medical product.
A 97% death rate among babies from pregnant mothers that were ‘vaccinated’ is appalling. And this was from Pfizer’s own clinical trial data. This suggests a massive breakdown in the health regulatory process. The public, whom health regulatory agencies are to be serving, should demand accountability from these government-run institutions.
If I were a regulatory scientist assessing the pregnancy outcome data from Pfizer, there is no way that I would ever have supported the use of their inoculation in pregnant women. And I would never have allowed ‘real-world’ data from flawed studies to replace proper pre-clinical and clinical trials. Nor would I remain silent about this knowledge. Regulators who know better need to start speaking up.

{kind=link}